
Dr. Phil Zeltzman’s Blog
From Florida to Pennsylvania: Mae Mae the Lab gets “a new lease on life” after tie back surgery for laryngeal paralysis
This may be one of my craziest success stories ever, and definitely my furthest traveling patient ever.
Mae Mae, a 10 year old Lab who had laryngeal paralysis (which we call “lar par”), was traveling from Florida to NY State with her owner.

As they arrived in Pennsylvania (where I live), Mae Mae had a severe bout of suffocation. Her owner contacted me after finding me on my website. His dog was in serious trouble.
In his own words: “We were on our way from Key West (FL) to The Adirondacks (NY). As we were driving through Harrisburg, PA, around 11 pm, Mae suddenly couldn’t breathe. Her lar par had, in an instant, gone from manageable to life threatening. Fortunately, we were close to a vet ER. They saved her life. They said she was very healthy and a good candidate for lar par surgery.”
“I sent you an email and was blown away to receive an almost immediate response and then a call. I knew then that Mae Mae was meant to be there in Pennsylvania at that moment and she was meant to live.”
We scheduled Mae Mae for emergency surgery at www.BrodheadsvilleVet.com. Surgery went well. She then recovered well with her owner.
“Great night sleep, for both of us. She’s doing well.”
But then it occurred. The dreaded complication happened: aspiration pneumonia. This is a type of pneumonia due to aspiration, or inhalation, of food, water, saliva or vomit into the lungs. Mae Mae was coughing and was extremely weak. She had no appetite.
She went to the local ER (www.BartonHeights.com).
“She spent a week in the ER. She had been through so much. She had literally given up. Because of COVID, I wasn’t allowed to see her. She was finally allowed in a private room where I spent half the day with her, every day. I would lay on the floor with her for 5 hours a day and try to get her to eat a little. Every day, she made a little more progress.”
It’s true. It looked as if Mae Mae had given up. She wasn’t fighting. So we fought for her. The doctor team and the nursing team did everything by the book to treat the pneumonia: antibiotics, nebulization, antibiotics, coupage, and lots of TLC.
Her biggest cheerleader was her owner. Despite the financial commitment and the emotional rollercoaster, he stood by her side, literally, as much as possible. In the end, Mae Mae recovered and finally continue her trip to the Adirondacks.
Her owner and I are convinced that she recovered thanks to the amazing dedication of one particular nurse, which we will call Shelly.
“Mae Mae is a special soul. You (Dr Zeltzman) and Shelly provided the best medical care I have ever experienced for pet or human. I will never be able to thank you enough.
Thank you for giving Mae Mae a new lease on life. Literally it has been like watching her be reborn. She is 10 years old and I am grateful I will get the opportunity to watch this precious soul grow old.”
Then Mae Mae travelled back home in Florida.
After 1 month, she was doing well, but was still pretty weak.

After 2 months, she is happy and much stronger, as shown in this short video: https://youtu.be/67WiKl9tpr4
Bottom line: “lar par is not a death sentence.” It’s a treatable condition. It has definite, well-known, possible complications. Even if we end up with aspiration pneumonia, most dogs who are treated aggressively can overcome this aggressive and potentially deadly complication.

Thanks to her owner’s amazing dedication, Mae Mae can breathe easy in Key West, where she enjoys a life of rest, walks on the beach, good food and puppy love.
Phil Zeltzman, DVM, DACVS, CVJ, Fear Free Certified

Dr. Phil Zeltzman is a traveling veterinary surgeon in Pennsylvania & New Jersey. An award-winning author, he loves to share his adventures in practice along with information about vet medicine and surgery that can really help your pets. Dr. Zeltzman specializes in orthopedic, neurologic, cancer, and soft tissue surgeries for dogs, cats, and small exotics. By working with local family vets, he offers the best surgical care, safest anesthesia, and utmost pain management to all his patients. Sign up to get an email when he updates his blog, and follow him on Facebook, too!
Laryngeal paralysis is not a death sentence
Laryngeal paralysis (aka “lar par”) is a common condition in dogs (and rarely cats). What follows are my thoughts about the condition, its treatment and its outcome. They are based on recent science, and many years of experience treating lar par.

What is Laryngeal Paralysis?
Laryngeal paralysis is a condition that severely affects a pet’s breathing.
In the veterinary world, we call it “Lar Par” in short. A few people call it LP.
The larynx (please note, it is larynx and not “lar-nynx” as many people call it…) is the medical name for the voice box. If you’ve ever had laryngitis, then your very own larynx was irritated. The larynx is also the entrance to the wind pipe (or trachea) and, beyond, to the lungs.
Besides making all kinds of noises, the job of the larynx is to close off after we inhale, open up when we inhale, and again shut off when we eat and drink so we don’t “swallow the wrong way.”
When laryngeal paralysis occurs, none of these things happen. Taking a deep breath becomes impossible. The poor dog literally suffocates.
Who can be affected?
The typical patient is an older large breed dog. The poster child is the Labrador.
Most dogs are over 10 years of age.
Males are affected 2-4 times more often than females.
There is a hereditary or congenital form of Lar Par, which can affect Bouviers des Flandres, Huskies and Dalmatians. In those rare cases, young dogs, 1 year or younger, are affected.
Lar Par has also been described in small to medium dogs, as well as cats.
To avoid posting a long list here, I’ve shared the list of breeds I’ve treated over the years at the bottom of this article*.
What happens?
Lar Par occurs because the nerves that control the muscles which act on the cartilages of the larynx are diseased.
Typically, the condition starts on one side (“unilateral” paralysis or hemiparesis). If your dog is an athlete or a working dog (racing, agility, police dog, serious hiking, Search And Rescue), you may notice breathing difficulties. But if your dog is a family pet or a couch potato, you probably won’t notice much.
Only when the condition affects both sides of the larynx (“bilateral” paralysis) will most pet owners realize that there is a problem.

What causes Lar Par?
Most of the time, we don’t know. This is called “idiopathic” Lar Par.
Occasionally, we find an underlying cause, such as hypothyroidism (a lazy thyroid). This is somewhat controversial, since hypothyroidism is common in older Labs and Goldens anyway. That said, treating hypothyroidism will never correct Lar Par. So we recommend treating hypothyroidism because of the other consequences, not because it helps or cures Lar Par.
Rarely, Lar Par is due to trauma, cancer, generalized diseases of nerves or muscles, or previous surgery (e.g. on the trachea or the thyroid gland).
What are the signs?
Lar Par is a very stressful condition for the patient — who obviously doesn’t understand what is going on. These dogs literally suffocate. It’s a terrible and terrifying condition.
Typically, the signs are progressive. The dog pants without exercising, has a noisy and labored breathing, and gets tired quickly during regular walks. Owners may notice that their dog’s voice changes and sounds hoarse.
Unfortunately, because Lar Par most often occurs in older dogs, the signs are often blamed on old age and arthritis… which delays treatment.
Therefore, Lar Par patients are often presented to a vet when they are in real trouble, i.e. when they can barely breathe. Most often, this happens as the weather becomes hot and humid, but I see these patients year-round, even in the Winter. Overweight or obesity worsens the condition.
At worst, the condition can become life-threatening.
How does my vet know my dog has Lar Par?
An experienced vet or surgeon will suspect Lar Par the second a patient walks into the exam room or on a 10 second video. But to confirm the suspicion, an exam of the larynx under sedation is necessary.
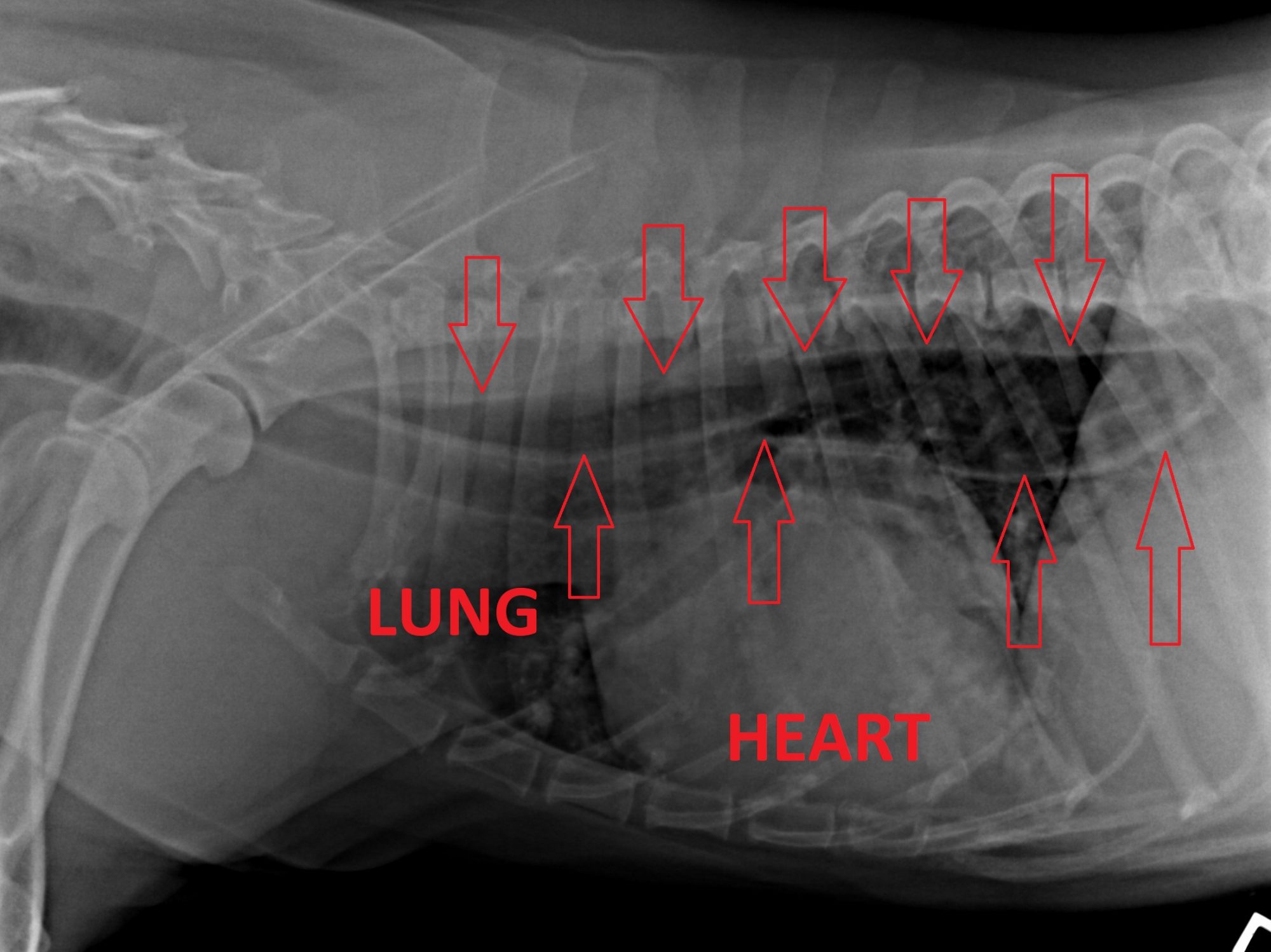
Before this can be done safely, we perform full blood work and chest X-rays. The purpose of blood work is to ensure the safety of sedation and anesthesia. The goal of chest X-rays is to know whether the patient has aspiration pneumonia (more on this below). The same X-rays can show if the patient as mega-esophagus, ie an enlargement of the esophagus – the tube between the mouth in the stomach. Finally, these X-rays confirm that there is no hidden cancer in the chest.
Under “light” sedation, the mouth is opened and the larynx is observed. With Lar Par, the folds of the larynx will not open and close as the patient breathes in and out. The folds remain closed – paralyzed.
Light sedation means that it should be heavy enough so the mouth can be opened, but mild enough for the patient to breathe spontaneously.

What is the emergency treatment?
When a patient presents on an emergency basis, two important goals are to calm the patient, and allow enough oxygen to get on board.
This requires sedation (acepromazine is often the drug of choice). Oxygen can be delivered by many different ways. In extreme cases, the patient needs to be anesthetized and a tube is placed down the throat to deliver oxygen.
My absolute least favorite way of stabilizing a Lar Par patient in crisis is an emergency tracheostomy, although it may be the only option in very rare cases.
If the patient’s temperature is seriously high from overheating, emergency measures are taken to lower it.
Once the patient is stabilized, surgery is the best treatment. Nothing else will work as successfully.
What happens in surgery?
The goal of surgery is to permanently open up the larynx to allow more air to get in.
There are two main types of surgery: intraoral (i.e. surgery is done via the mouth) and extraoral.
These days, the vast majority of surgeons will choose the extraoral approach, i.e. surgery is done through the left side of the neck. Most often, they will typically do a laryngeal “tie-back” procedure, a.k.a. arytenoid lateralization, on ONE side.
Typically, surgery involves placing 2 heavy nylon sutures (i.e. permanent) to open up the left side of the larynx. Only one side (again, typically the left) is opened up to minimize the risk of aspiration pneumonia.
Doing surgery on both sides dramatically increases the risk of aspiration pneumonia… and is simply not necessary.

What is the outcome?
In good hands, the outcome is typically good.
Theoretically, surgery provides instant relief: The patient can finally breathe. Then of course (s)he needs to recover and heal after surgery.
Clients often worry about doing this surgery in their (typically) older dog. The fact is, more lar par patients are over 10 years old.
My standard replies are:
1. Age is not a disease.
2. Lar Par is not a death sentence. It’s a bump along the road, which shouldn’t affect the patient’s life expectancy as long as they don’t get deadly aspiration pneumonia.
What are the complications?
. Coughing is expected after surgery, typically after eating and mostly after drinking. That’s a good thing, as it will hopefully prevent the dog from “swallowing the wrong way.”
. The voice may change, and barking disappears. These are not really complications. They are standard consequence of the tie back procedure you need to be aware of.
. Failure of the nylon sutures and/or a condition of the cartilage of the larynx (too soft or too brittle) are rare but severe complications, which is why we insist on confinement, peace, and quiet after surgery.
. The dreaded complication is Aspiration Pneumonia (also known as AP). This is a type of pneumonia due to aspiration, or inhalation, of food, water, saliva or vomit into the lungs. Thankfully it is an uncommon complication.
. GOLPP (geriatric onset laryngeal paralysis polyneuropathy) is not really a complication of lar par, but something to be aware of, especially in Labs. More information can be found here:

What if my pet gets aspiration pneumonia? Then what?
It’s crucial that aspiration pneumonia is caught early.
It is an aggressive disease that must be treated aggressively.
We look for 4 criteria: coughing, lethargy, poor appetite and a fever.
If you ever suspect AP, time is of the essence. A vet should see the patient ASAP, listen to the lungs and take chest X-rays to confirm the diagnosis. Treatment involves hospitalization, IV fluids, strong antibiotics, nebulization and a type of physical therapy called coupage.
What’s new with Laryngeal Paralysis?
We now give patients 2 anti-vomiting drugs (metoclopramide and Cerenia) and an antacid before surgery.
Then they stay on cisapride (a daily pill) for life, after surgery. The hope is to decrease the risk of vomiting by helping move food downward.
These days, we don’t make the opening in the larynx as big as we used to, just enough for the patient to breathe comfortably. This is clearly art more than science, and you can see how experience comes into play. What’s the downside? The patient will likely have a noisier breathing, as air goes through a smaller opening. But again, as long as the patient can breathe comfortably, we don’t mind. As I always tell my clients, “I don’t treat noise, I treat dogs.”

What do I need to do at home after surgery?
This will depend on your surgeon’s recommendations. In my practice, we recommend:
• Strict rest for 2 months to allow proper healing with scar tissue
• Soft food (“meat balls”) for 2 weeks
• Not too much water intake at once
• Pain killers for 7 days
• Cisapride for life (not all surgeons do that)
• Weight loss (these patients are often chubby), or weight control as needed
• A harness instead of a neck collar
The only restriction is swimming: your dog will have a permanently open larynx, with no possibility of closing it off, should (s)he swallows water. There is therefore a risk of aspiration at best, and drowning at worst.
What’s the bottom line?
Overall, Lar Par is a stressful condition for the dog and a stressful situation for the owner. Fortunately, in most cases, results of Laryngeal Paralysis surgery are good to excellent.
Phil Zeltzman, DVM, DACVS, CVJ, Fear Free Certified
* Here is a list of breeds I’ve treated over the years:
Labradors and Lab mixes are # 1 by very very far.
Golden retriever
Pitbull
Greyhound
Shepherd (and mixes)
St. Bernard
Britany spaniel
Husky (young or old)
Sheltie
Beagle
Akita
Mastiff
Boxer
Bulldog (yes, really)
Pomeranian
Wheaten Terrier
Border collie
Springer spaniel
Chessie (Chesapeake Bay Retriever)
Bassett hound
Dr. Phil Zeltzman is a traveling veterinary surgeon in Pennsylvania & New Jersey. An award-winning author, he loves to share his adventures in practice along with information about vet medicine and surgery that can really help your pets. Dr. Zeltzman specializes in orthopedic, neurologic, cancer, and soft tissue surgeries for dogs, cats, and small exotics. By working with local family vets, he offers the best surgical care, safest anesthesia, and utmost pain management to all his patients. Sign up to get an email when he updates his blog, and follow him on Facebook, too!
What is GOLPP (Geriatric Onset Laryngeal Paralysis Polyneuropathy)?
We used to believe that laryngeal paralysis was a standalone condition. Recent research shows that it’s a bit more complicated. Laryngeal paralysis is a disease of the nerves (poly-neuropathy) that can sometimes affect other body parts besides the larynx (voice box).

What is GOLPP?
To better describe this complicated disease, it was named Geriatric Onset Laryngeal Paralysis Polyneuropathy (GOLPP in short). GOLPP slowly gets worse over time. It affects dogs developing signs of upper airway obstruction or blockage.
It has been observed in older or geriatric dogs, particularly in Labrador retrievers and other large breed dogs. We now understand that there are 3 main parts to this disease.
* 1st condition: laryngeal paralysis
Affected dogs are most often brought into the hospital because of signs associated with laryngeal paralysis, because it’s the most obvious one and can be life-threatening. It causes dogs to have difficulty breathing, to the point that they can suffocate.
For more information on lar par, click here: Laryngeal paralysis is not a death sentence
* 2nd condition: mega-esophagus
Further questioning may reveal “spitting” up food, sometimes mistaken as vomiting (which is very active, ie lots of effort).
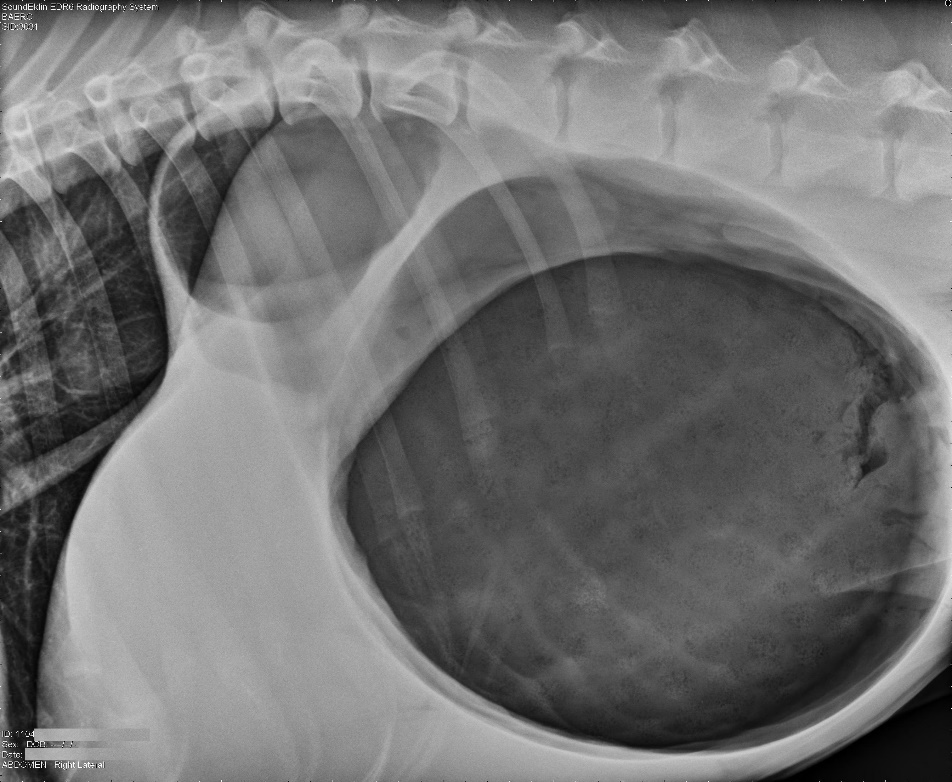
Because there is no effort involved, the condition is called regurgitation. It is due to a malfunction of the esophagus, which is the tube between the mouth and the stomach. It becomes extremely distended (mega-esophagus) and food simply piles up inside, instead of going down into the stomach. When the amount in the esophagus is too much, it’s expelled effortlessly via regurgitation.
This increases the risk of aspiration pneumonia since these dogs have trouble protecting their airways and lungs.
* 3rd condition: back leg weakness
In addition, some dogs develop weakness in their back legs. Sadly, it is often inaccurately blamed on arthritis or old age.
In reality, it really has to do with the same nerve condition. The legs are not well coordinated, and the muscles get weaker over time.
Which breeds are affected by GOLPP?
Most of the research has been done in Labradors. We know for a fact that Labs can get GOLPP. Some authors say that they all get it eventually. I think that it’s a bit more nuanced than that. I don’t think they all get it.
The condition has also been diagnosed in other purebreds and mixed breeds, but there isn’t as much research about them.
What is the treatment of GOLPP?
There is no cure for GOLPP, but there are ways to help each one of its components.
The gold standard to treat laryngeal paralysis is surgery (called a tie back). In good hands, i.e. typically those of an experienced board-certified surgeon, it provides good results as it allows the patient to breathe and function. Despite possible complications, surgery dramatically increases both lifespan and quality of life.
There is no treatment for megaesophagus per se. The dog needs to be fed soft to liquid food, then remain upright for 15 minutes after each meal.
Dogs with weak back legs benefit from slow leash walks and physical therapy to strengthen the muscles.

What should you do if your dog has GOLPP?
As a surgeon who deals with laryngeal paralysis & GOLPP frequently, this is what I tell my clients. Other surgeons may disagree, so please understand this is my personal & professional opinion, based on years of experience.
The best way to help a dog with laryngeal paralysis is surgery (a tie back). Suffocating is a horrifying way to live. Of the 3 different components of GOLPP, lar par is the one that affects quality of life the most, and the only one we can “fix.”
So my (again, personal) philosophy is: fix what can be fixed, and be ready to deal with what cannot be fixed (megaesophagus and weakness). It’s not for everybody. It requires serious love and dedication.
If the dog has megaesophagus at the time of the diagnosis, it still may not preclude performing surgery. It definitely increases the risk of aspiration pneumonia, but several of my most dedicated clients have helped their dogs successfully.
If the dog has a weak backend, at least this part is not life-threatening in the short term. With proper exercise and physical therapy, we can still help these dogs. And chances are, once a weak dog finally gets more oxygen, (s)he might get stronger after a tie back.
Ultimately, by putting together the right treatment plan and the right team, which includes a very loving and dedicated pet owner, affected dogs can maintain a good quality of life.
Phil Zeltzman, DVM, DACVS, CVJ, Fear Free Certified
Dr. Phil Zeltzman is a traveling veterinary surgeon in Pennsylvania & New Jersey. An award-winning author, he loves to share his adventures in practice along with information about vet medicine and surgery that can really help your pets. Dr. Zeltzman specializes in orthopedic, neurologic, cancer, and soft tissue surgeries for dogs, cats, and small exotics. By working with local family vets, he offers the best surgical care, safest anesthesia, and utmost pain management to all his patients. Sign up to get an email when he updates his blog, and follow him on Facebook, too!
What causes bloat?
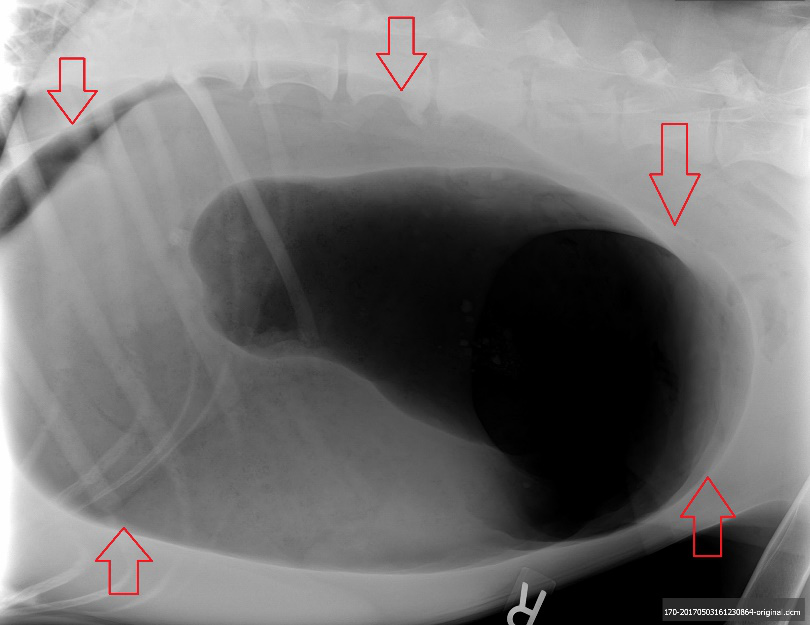
“Bloat” is also called many different things: twisted stomach, Gastric Dilatation Volvulus (GDV), gastric torsion, stomach torsion etc.

Side note: it’s unfortunate that we (vets and dog owners) have gotten used to calling it bloat. After all, bloating is not a big deal in people. Yet “bloat” can kill a dog in a matter of hours.
Vets sometimes tell pet owners that we don’t really know what causes GDV, and therefore we don’t know how to prevent it. However, that is not exactly accurate…
Here is a summary of the main known causes.
1. Breed
Large and giant dog breeds are at risk for GDV, including Great Danes (the #1 breed), German shepherds, Weimaraners, St. Bernards, Dobemans and Old English sheepdogs. These breeds are roughly 25% more likely to get GDV than others.
A few smaller breeds, such as basset hounds, boxers, and standard poodles can also be prone to GDV.
2. Conformation
Conformation has to do with the shape of a dog.
Dog breeds called “deep-chested,” have a tall chest and a skinny belly. Think of a Great Dane. A deep chest, combined with stretching of ligaments that attach to the stomach, increases the chance of stomach torsion.

3. Genetics
Dogs with a first-degree relative who had GDV are at greater risk of getting
it themselves. This chance increases by 20% with each additional year. These factors confirm that GDV is a partially genetic disease and dogs at risk should be spayed or neutered.
In addition, better selection should be taken seriously by breeders.
4. Stress
Stressful situations can also contribute to a twisted stomach. Boarding, thunderstorms, moving, vet visits and hospitalization are all potential triggers for nervous dogs.
One study showed that having a high-stress environment or being fearful contributed to GDV compared to similar dogs who were in a non-stressful environment.
5. Feeding
Eating fast, and how often dogs are fed, have been shown to increase the risk of stomach torsion.
Therefore, if your dog eats fast, it’s important to find ways to slow it down. There are special bowls made for that purpose.
In addition, dogs fed once per day are more likely to have GDV, compared to dogs who are fed 3 times daily. Several small meals throughout the day are better for dogs at risk.
6. Food
Believe it or not, studies have shown that moistening dry dog food before feeding actually increases the risk of GDV in large-breed dogs.
Ironically, feeding a dry-only diet has also been shown to increase risk.
So what’s a concerned dog owner to do?
Recommendations have been made to help prevent a first episode by avoiding exclusively dry, expanded, cereal-based, or soy protein-based commercial dog foods.
Feeding a combination of dry and canned food together may be a way to lower the chances of GDV. I insist: “may be a way.” There are no guarantees here, only ways to try to lower the chances.
Also, foods with fat listed among the main 4 ingredients have been shown to increase the risk of GDV. So please look at the list of ingredients on your dog food.

7. Water
It is recommended to avoid drinking large amounts of water before and after exercise.
Ironically, too little water before and during meals may increase the chance of a dog suffering from GDV! A recurring “hot story” about ice water causing GDV regularly shows up online and appears to be a complete hoax.
8. Exercise
A fairly classic recommendation to reduce the risk of stomach torsion is to avoid heavy exercise 1 hour before and 2 hours after eating a meal. The idea is that it’s easier for a stomach to twist when it’s full compared to when it’s (partially) empty.
9. Age
Even though I always say, “age is not a disease,” age can play a role in a dog’s risk for stomach torsion.
In Great Danes specifically, age is a very important risk factor for GDV.
One of the reasons may be the stretched ligaments, over time, as mentioned above.
10. Other risk factors
There are countless other risk factors that are unproven, controversial, or contradicting.
. For example, some studies show that a raised bowl is better to decrease aerophagia (aka swallowing air), while others imply a bowl on the floor is ideal.
. The at-risk gender varies from study to study.
. The month, the cycle of the moon, and a previous spleen removal are also fuzzy risk factors.
- Gastropexy
This last point is not a risk factor – on the opposite, but it’s important to mention here.
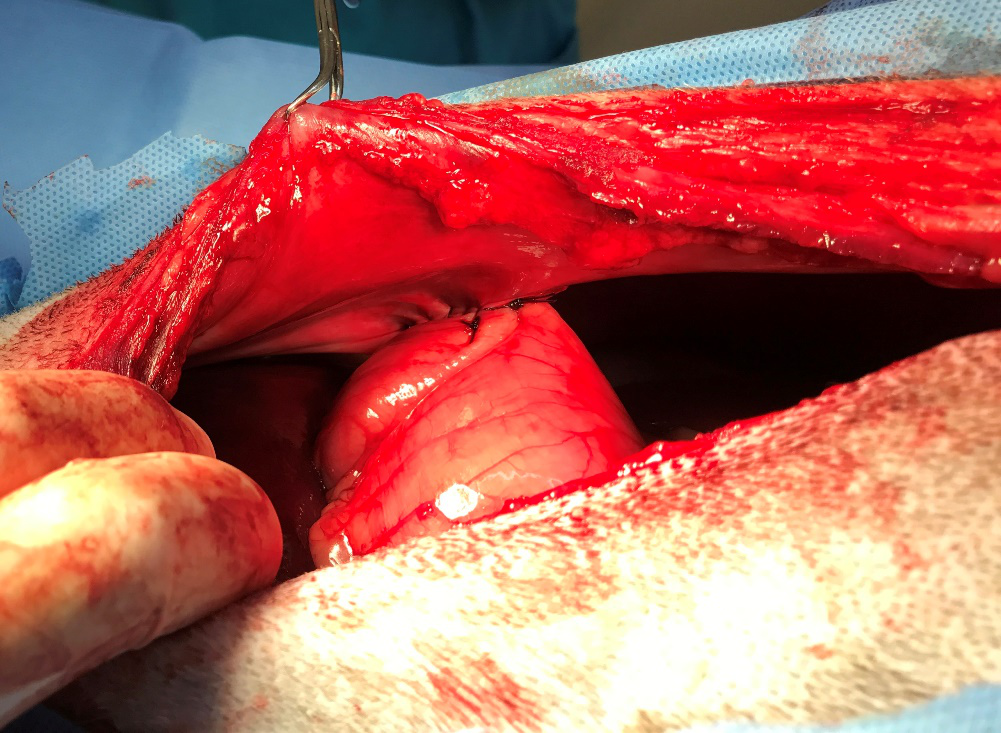
A gastropexy, or tacking the stomach to the inside of the belly, is a simple surgery that can prevent twisting of the stomach. In good hands, it’s successful over 95% of the time.
Importantly, it prevents twisting of the stomach, not true “bloating” – aka the stomach getting full of air – we don’t know how to prevent that and it remains a risk for life.
The gastropexy or “pexy” in short is part of the surgery to treat GDV. But it can also be done preventively, or prophylactically. So it’s called a prophylactic gastropexy.
For example, Great Danes have a 40 % chance of having GDV in their lifetime. Ideally, this life-saving surgery should be performed at the time of the dog’s spay or neuter – or as soon as possible after that. Of course, it’s never too late to prophylactically pexy a dog… until they have an episode of GDV.
Please beware, the next picture of a gastropexy can seem graphic to some readers.
I have helped a number of pet owners perform gastropexies over the years. Some were wise to do it before GDV happens in their at-risk dog. Some learned the hard way (i.e. their dog got a twisted stomach, and that’s how they learned about the pexy option).
Either way, it can be done as a “stand alone” surgery, or at the time of a spay or neuter.
To recap, we know a lot about the risk factors of GDV. Be aware of them, and prevent those you can control. You could very well save your dog’s life.
Phil Zeltzman, DVM, DACVS, CVJ, Fear Free Certified
Dr. Phil Zeltzman is a traveling veterinary surgeon in Pennsylvania & New Jersey. An award-winning author, he loves to share his adventures in practice along with information about vet medicine and surgery that can really help your pets. Dr. Zeltzman specializes in orthopedic, neurologic, cancer, and soft tissue surgeries for dogs, cats, and small exotics. By working with local family vets, he offers the best surgical care, safest anesthesia, and utmost pain management to all his patients. Sign up to get an email when he updates his blog, and follow him on Facebook, too!
Should you wait to get help for your pet?

Your pet is vomiting. Should you wait to go to the vet?
Your pet is limping. Should you wait to seek help?
Your pet has a mass. Should you wait to have it looked at?
These are common dilemmas, and the answer is… it depends!
Let’s keep our 3 examples.
. Many pets vomit every once in a while, and they are perfectly healthy otherwise.
Other times, repeated vomiting is a sign that something is brewing inside. And it could be anything: stomach problems, intestinal conditions, kidney disease, cancer etc.
. Some pets limp because of a sprain and get over it by the next day, just like a human.
Other times, ongoing limping is a sign of a problem: elbow arthritis, hip dysplasia or the most common cause of limping: a torn ACL.
. Many pets have skin masses. Most masses can only do one thing: get bigger. Very rarely does a mass get smaller. It would defy science: as cells divide, which they are genetically programmed to do, the mass gets bigger. It can be slow or it can be fast, but they usually get bigger over time. The only way to objectively know what is going on is to measure it.
So what’s a pet lover to do?
Should you keep an eye on it?
For a short while, possibly.
Waiting any longer is rarely a good idea.
. Repeated vomiting can lead to dehydration and electrolytes imbalances.
. An untreated joint problem invariably leads to arthritis, which can only get worse over time.
. A small mass is easier, less invasive and cheaper to remove than a large mass. This translates to longer anesthesia, higher surgery fees and higher chances of complications.
Occasionally, you will be a bit early and it’s a false alarm.
Most times, you will be right and acting early will save you time, money and frustration while avoiding pain for your pet.
At the very least, call your vet to ask questions. Many vets now offer telemedicine consultations, which means you don’t even have to take your pet to the vet. You can get advice from the comfort of your home.
Just keep in mind that vomiting may require X-rays or an ultrasound, limping may require X-rays and a mass may require lab testing.
Either way, don’t procrastinate, it rarely leads to good results.
Phil Zeltzman, DVM, DACVS, CVJ, Fear Free Certified
Dr. Phil Zeltzman is a traveling veterinary surgeon in Pennsylvania & New Jersey. An award-winning author, he loves to share his adventures in practice along with information about vet medicine and surgery that can really help your pets. Dr. Zeltzman specializes in orthopedic, neurologic, cancer, and soft tissue surgeries for dogs, cats, and small exotics. By working with local family vets, he offers the best surgical care, safest anesthesia, and utmost pain management to all his patients. Sign up to get an email when he updates his blog, and follow him on Facebook, too!